
CHARLESTON, W.Va. — A West Virginia physician and former law-enforcement officer is urging state leaders to invest in a chronic care hospital aimed at treating the mentally ill, drug addicted, and homeless.
“This is not only a West Virginia issue, but a national one, and it is nonpartisan,” Dr. Norman Wood said in a written statement shared with state officials. “And to date, for the past 40 years, we have not been dealing with this in any sense that has brought about success.”

Wood has shared his proposal with members of the governor’s staff and lawmakers, presented it on Dec. 2 to Parkersburg Mayor Tom Joyce in the presence of Sen. Mike Azinger, and delivered versions of the message multiple times to the Wheeling City Council.
He frames the approach as both a public-health intervention and an economic-development necessity, arguing that West Virginia’s reputation is being damaged by addiction, mental illness, homelessness, and incarceration.
“These very public tragedies have not only sucked the life out of our communities,” he said, “but they have given West Virginia the terrible image of being a state of backward people who are not smart enough to end their own addictions to narcotics or address their mental illnesses.”
The state should “take a portion of the opioid money” and build what he calls a “New Hope” state hospital where people in the mentally ill, drug addicted, and homeless population will finally get the help they have been praying for.
“The Governor and Legislature have the opportunity to take a portion of the opioid money and use it for the very families who earned that money on their own backs,” Wood said, referring to the opioid settlement he credited to Gov. Jim Justice’s efforts as attorney general. “Now let’s build on that success.”
“We can’t arrest our way out of this problem.”
Wood argued that incarceration has become the state’s default response to addiction and mental illness and said it is failing. “We can’t arrest our way out of this problem,” he says
Wood previously served as the physician director for the W.Va. Division of Corrections and Rehabilitation, where he helped develop medical service contracts for 24 state facilities and became familiar with the care provided to incarcerated people.
He described what he called a considerable overlap between incarceration, drug addiction, and mental illness.
“We are looking at more than 80 percent of our inmate population that are mentally ill, drug addicted, or both,” he said, citing his estimate that more than 60 percent of inmates have a substance use disorder diagnosis and 10 percent have what he described as severe mental illness.
A hospital-based alternative, he says, would give judges and prosecutors “more options on sentencing” and, for some individuals, allow part or all of a sentence to be served in a facility designed for long-term treatment.
“For qualified individuals, they could serve part or whole of their time in a hospital where they would have a greater chance of leaving that facility and joining society as a contributing member,” Wood said, “and not as a burden on the state.”
Closing camps is “a necessary first step.”
Wood also described homelessness as primarily driven by untreated mental illness and addiction, not simply a lack of housing.

“This is not a housing problem; this is a mental health and addiction problem,” he said. “These people had mental health issues or drug addictions long before they became homeless. The reason they are homeless is because of their mental illness or addictions.”
In Wheeling, Wood said he advised local leaders that closing a homeless camp was “the necessary first step to clean up their town,” and he described conditions he observed at a camp he visited in the spring.
“These people have no source of heat, warm food, or any sanitation,” he said. “They are a danger to themselves, and they can't help it.”
Wood said he believes the overwhelming majority of people in homeless camps are struggling with mental illness, addiction, or both, and he argued that many will refuse voluntary help because their illnesses prevent insight or consistent decision-making.
“Many of the homeless have anosognosia where their brains are not capable of recognizing that they have a problem,” he said. “They will take handouts, but they will refuse any real help in just about every way.”
Criticism of “warm and fuzzy” approaches
Wood sharply criticized models he characterized as outpatient-focused—including community detox, short-term rehab, social services, and some nonprofit approaches—calling them well-intentioned but ineffective for the population he is describing.
“All of these warm and fuzzy feeling efforts of community detox centers, social services, and housing will never make a dent,” he said. “They do not understand the root problem.”
He argued that decades of short-term treatment approaches have not reversed the trend. “Can anyone honestly say we are doing better now than we did 40 years ago?” Wood said. “That answer is no.”
He also alleged that some organizations profit from cycles of relapse and instability, describing some as using the population as “their personal ATM.” Those statements reflect Wood’s claims; he did not provide documentation in the material he shared.
“If you are not putting money towards a new chronic care state hospital,” he said, “you are throwing that money away, and you are allowing people to die.”
“We now know why,” he says, pointing to brain imaging
Central to Wood’s proposal is his assertion that addiction changes the brain in ways that make short-term treatment ineffective and that modern brain imaging will help prove when recovery is underway.
“We now know that narcotics, including marijuana, have neurotoxic effects on the brain, especially the prefrontal cortex,” Wood said. “The prefrontal cortex is turned off by narcotics.”
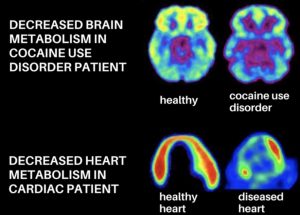
Wood said functional imaging, such as fMRI and PET scans, can demonstrate damage and track recovery, and he argued that the timelines involved are far longer than typical rehab stays.
“With Dr. Goldstein’s research, we can now prove that it takes the brain three to four months just to start to heal after abstinence,” he said, “and it takes up to two years for the brain to recover.”
That's why “the 30-to-90-day inpatient drug detox and rehab clinics are failing and will never work,” he said.
In the materials he shared, Wood said he has been communicating with Dr. Rita Goldstein of the Icahn School of Medicine at Mount Sinai and claimed she would help design a program in West Virginia if a long-term hospital were created.
“She is all in on helping us set it up so we can properly do our brain scans to determine damage and healing,” Wood said.
Wood argued that showing patients their own progress through imaging could strengthen motivation before release.
“We can now truly say to a person who has struggled for years with addiction that they are actually getting better,” he said, “and they can see it with their own two eyes in reviewing these scans.”
A long-term state hospital model
Wood’s bottom line is a treatment model that lasts years, not weeks, including what he describes as chronic care for addiction and severe mental illness, and potentially for some incarcerated people before release.
“If we are going to have any chance of helping these people,” he said, “they must be in a state hospital for up to two years if not three.”
He described the stakes in emotional terms, repeatedly returning to the impact on families.
“In West Virginia, there will be three mothers screaming today in floods of tears, why wasn’t there some way to save their babies?” Wood said. “There were three mothers yesterday, and there will be three mothers tomorrow.”
He added, “I have never met a mother who wouldn’t want to visit their child in a hospital over a cemetery.”
Personal experience and case examples
Wood grounded his solution in what he described as decades of experience across law enforcement, medical practice, and corrections, saying that background gives him an unusual view of what he calls the “true nature” of the mentally ill, drug addicted, and homeless population, which he has termed "MIDAH."
“I know these people better than anyone else you will talk to,” he said. “That’s a bold statement, but I can back it up.”
He recounted work he said he performed in outpatient settings, including efforts to stabilize people with schizophrenia through medication management, describing those successes as rare without a controlled, long-term environment.
“For the vast majority of the mentally ill, drug addicted, and homeless, you will be lucky to see them twice in an outpatient setting in a year,” he said. “An outpatient setting will never work for the mentally ill, drug addicted, and homeless, and they haven’t in 40 years.”
Wood also described a personal loss involving a patient who died from an overdose after a period of treatment, using it as an example of why he believes existing models fail families.
“These are the most important points to remember,” he said. “They can’t stop on their own, and an outpatient setting will never work. And it takes the brain two to three years to recover after a narcotic addiction.”
“This will never end” without significant change
However, he says, the state’s opioid settlement offers an opportunity to create a nationally watched model if leaders choose a more restrictive and long-term approach than what he believes has been tried for decades.
“If you want every other state to look at West Virginia in awe, we need to do this,” he said. “West Virginia can lead the nation in this effort.”
Without that change or a move toward a state hospital approach, he warned, the cycle will continue. “This problem takes the resolve and fortitude to do what is needed,” he said. “If we don’t, this problem will never get any better, and mothers will cry forever.”
Quick facts about the New Hope proposal
What’s being proposed?
A new state hospital, “New Hope,” a chronic-care facility for people who are mentally ill, drug addicted, and homeless—a group the doctor terms "MIDAH."
Who is proposing it?
Physician and former law-enforcement officer Dr. Norman Wood, who says he has treated thousands of people in the mentally ill, drug addicted, and homeless population over five decades.
Why now?
Wood says 40 years of short-term treatment, housing programs, and incarceration have failed, while addiction, homelessness, and overdose deaths have worsened.
How would it be funded?
By using a portion of West Virginia’s opioid settlement funds, which Wood says were “earned by families through loss and suffering.”
What’s different about this approach?
Long-term care—two to three years if needed—instead of 30- to 90-day detox or rehab programs, which Wood says “will never work.”
Why long-term treatment?
Wood says brain imaging shows it takes months for the brain to begin healing after drug use and up to three years for meaningful recovery, especially in the prefrontal cortex.
Who would be treated there?
People with serious mental illness, substance-use disorder, homelessness, and some incarcerated individuals are considered before release.
What problem is it meant to fix?
Wood argues West Virginia “can’t arrest its way out” of addiction and mental illness and that prisons are not equipped for individualized care.
What’s the goal?
To help people leave treatment drug-free, mentally stable, housed, employed, and out of the criminal justice system.
Why does Wood say current efforts fail?
He says outpatient clinics, short-term rehab, and housing programs treat symptoms, not causes, leading to relapse and repeated crises.
What does he say is at stake?
“I have never met a mother who wouldn’t want to visit their child in a hospital over a cemetery.”
In 1988, Dr. Norman Wood was a special agent with the U.S. Customs Service. After an almost a year-long undercover investigation, he seized the ocean-going tug boat Intrepid Venture, towing a drug-filled barge under the Golden Gate Bridge, San Francisco, Calif.
Sign up to receive a FREE copy of West Virginia Explorer Magazine in your email weekly. Sign me up!

{kind=link}